An introduction
Ecstasy has to be one of the most talked-about drugs in the media, but it might surprise you to learn that it's been around since 1914, when it was manufactured by the pharmaceutical company, Merck. It was classified as an illicit substance in the UK in 1977, and in the US in 1985, but prior to that it was widely used as an adjunct to psychotherapy due to its perceived ability to lower defensiveness and promote empathy.
It first began to gain notoriety in the 1990s, with the advent of the rave scene, and the toxic effects associated with the drug have been highly publicized. However, there are some that feel that its dangers are grossly overestimated (for example, see here) and that ecstasy is the victim of a media publishing bias. While there may be some truth in this, and for sure many individuals continue to take ecstasy without any serious adverse side-effects, animal and human studies have repeatedly shown that the drug can induce toxic-like alterations in the brain, specifically within the serotonergic system. Serotonin plays a vital role in the regulation of mood and homeostatic mechanisms, including feeding and sleeping. The serotonergic system is the primary target of many antidepressants such as Prozac, which has caused researchers some alarm, as ecstasy consumption - while having no apparent short-term effects - could cause later problems such as depression and anxiety that may not be amenable to the usually prescribed pharmacotherapies. As ecstasy use only became widespread in the 1990s, it could be some time before we know for sure what its long-term effects are.
Some caveats:
It has to be kept in mind that dosage is critical in ecstasy research: animal studies use pure MDMA (the chemical name for ecstasy is 3,4-methylenedioxymethamphetamine; more about that later!), while ecstasy tablets contain indiscriminate amounts of the drug. In addition, the phenomenon of inter-species scaling can be applied to MDMA, whereby animals that are smaller in size actually require MORE drug than larger animals, to have the same effect. Therefore, we must be very careful when conducting MDMA research in animals, to ensure that doses used are effectively comparable to human consumption. Another problem in animal research is that the drug is metabolized a little bit differently, which should also be kept in mind. Most interestingly, MDMA has a completely different neurotoxicity profile in the mouse, compared to rats and non-human primates, and appears to target the dopaminergic system rather than serotonin. Therefore, data from mouse studies cannot be extrapolated to what is observed in other laboratory species.
It first began to gain notoriety in the 1990s, with the advent of the rave scene, and the toxic effects associated with the drug have been highly publicized. However, there are some that feel that its dangers are grossly overestimated (for example, see here) and that ecstasy is the victim of a media publishing bias. While there may be some truth in this, and for sure many individuals continue to take ecstasy without any serious adverse side-effects, animal and human studies have repeatedly shown that the drug can induce toxic-like alterations in the brain, specifically within the serotonergic system. Serotonin plays a vital role in the regulation of mood and homeostatic mechanisms, including feeding and sleeping. The serotonergic system is the primary target of many antidepressants such as Prozac, which has caused researchers some alarm, as ecstasy consumption - while having no apparent short-term effects - could cause later problems such as depression and anxiety that may not be amenable to the usually prescribed pharmacotherapies. As ecstasy use only became widespread in the 1990s, it could be some time before we know for sure what its long-term effects are.
Some caveats:
It has to be kept in mind that dosage is critical in ecstasy research: animal studies use pure MDMA (the chemical name for ecstasy is 3,4-methylenedioxymethamphetamine; more about that later!), while ecstasy tablets contain indiscriminate amounts of the drug. In addition, the phenomenon of inter-species scaling can be applied to MDMA, whereby animals that are smaller in size actually require MORE drug than larger animals, to have the same effect. Therefore, we must be very careful when conducting MDMA research in animals, to ensure that doses used are effectively comparable to human consumption. Another problem in animal research is that the drug is metabolized a little bit differently, which should also be kept in mind. Most interestingly, MDMA has a completely different neurotoxicity profile in the mouse, compared to rats and non-human primates, and appears to target the dopaminergic system rather than serotonin. Therefore, data from mouse studies cannot be extrapolated to what is observed in other laboratory species.
The substituted amphetamines
Ecstasy is classified as a substituted amphetamine. Amphetamine and its derivatives are unique in that they do not exist in nature and are entirely synthetic substances. Structurally, they resemble the neurotransmitters noradrenaline and dopamine, which accounts for their pharmacological properties and subsequent behavioural effects. These drugs are psychostimulants, and produce feelings of euphoria that are mediated by dopamine - brain levels of this neurotransmitter are increased by all drugs of abuse, and it is this increase that is responsible for the rewarding effects or pleasurable 'high' - and induce high levels of motor activity, which are driven by noradrenaline and dopamine. However, they can also cause anxiety due to overactivation of the stress mechanisms of the body (similar to caffeine jitters), and in a minority of susceptible individuals, can induce serious cardiovascular distress or even seizures.
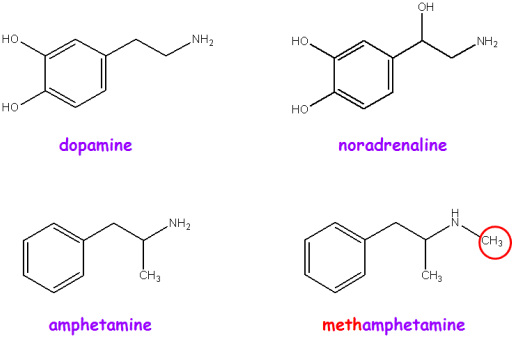
The structural similarities between amphetamine and methamphetamine ('crystal meth'; so-called because of the addition of a methyl group - CH3 - to the basic amphetamine structure) and the neurotransmitters dopamine and noradrenaline. Such structural similarities allow the drugs to mimic the effects of these neurotransmitters
MDMA differs from amphetamine and methamphetamine in that it also structurally resembles serotonin. This probably accounts for its empathetic and emotional features, and its sometimes reported hallucinogenic-like effects (the serotonin system is also the target of hallucinogenic drugs such as mescaline and LSD - as an aside, serotonin is very important in 'gating' sensory information that we receive from our external environment. Hallucinogenics interfere with this process and hence, drugs such as LSD seem to increase perception of the world around us and cause 'merging' of the senses - for example, 'seeing' music, and 'hearing' colours). Ecstasy therefore has the dual effects of a serotonergic-based hallucinogen and a noradrenaline/dopamine-based psychostimulant.
This is made possible by the addition of a methylenedioxy group to methamphetamine, resulting in methylene(M)dioxy(D)meth(M)amphetamine(A). The 3,4 refers to the positioning of the methylenedioxy group, and how it is attached to methamphetamine.
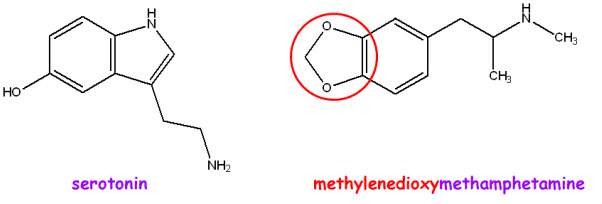
The structural similarity between MDMA and serotonin; particularly note the 5-sided methylenedioxy group that resembles the 5-sided group in serotonin. This is attached to the 3rd and 4th carbons of the 6-sided benzene ring to give 3,4-methylenedioxymethamphetamine
What does ecstasy do?
MDMA brings about increased levels of serotonin, noradrenaline, and dopamine in the synaptic cleft (the synaptic cleft is the junction between two nerve cells and acts to relay signals within the nervous system). Its effects on serotonin are especially profound, resulting in massively high levels of the neurotransmitter, which is followed by its clearance and short-term depletion, leading to the 'post-ecstasy blues' or depression-like symptoms that are common for several days after ecstasy consumption.
In addition to its more long-term effects on the brain (see Introduction), which result from repeated exposure to the drug, there are four principal types of acute toxicity associated with ecstasy consumption, according to Kalant (2001). These can present after taking just one tablet:
Number 4 is probably the most dangerous type of toxicity and is the greatest contributor to a fatal outcome. It is also the most studied type of toxicity, and I will now go into more detail about its origins.
In addition to its more long-term effects on the brain (see Introduction), which result from repeated exposure to the drug, there are four principal types of acute toxicity associated with ecstasy consumption, according to Kalant (2001). These can present after taking just one tablet:
- Hepatic, referring to the liver, which is possibly related to metabolism of the drug
- Cardiovascular, which includes increased heart rate and blood pressure
- Cerebral, referring to the brain, whereby excessive water intake and occasionally, inappropriate hormonal release, results in swelling that can induce seizures and compression of the brainstem and cerebellum that interferes with respiration and circulation
- Hyperpyrexic, referring to increased body temperature, which includes breakdown of skeletal muscle cells (see below) due to overexertion and release of their contents into the bloodstream, leading to subsequent kidney failure. Fever can also cause liver damage and widespread blood clotting.
Number 4 is probably the most dangerous type of toxicity and is the greatest contributor to a fatal outcome. It is also the most studied type of toxicity, and I will now go into more detail about its origins.
MDMA and thermoregulation
My scientific interest in ecstasy goes back to my PhD days, when I investigated its toxic effects in rats, concentrating on the body temperature response and also, its impact on the serotonergic system. These are intrinsically connected: one of the main effects of MDMA is to increase core body temperature, which is essential for serotonergic neurotoxicity to occur. This body temperature response to MDMA is absolutely fascinating, as it is entirely dependent on ambient temperature: high ambient temperatures lead to hyperthermia (increased body temperature), while low ambient temperatures result in hypothermia (decreased body temperature). Another interesting aspect is the issue of aggregation toxicity: in laboratory animals, group-housing increases the hyperthermic effect of MDMA, while singly-housing increases the threshold for a hyperthermic response (i.e., greater doses of MDMA are required to produce hyperthermia). [This is especially relevant to human consumption of MDMA, which typically takes place in a hot and crowded environment - interestingly, ambience also hugely affects the MDMA behavioural response, and users report an entirely different subjective experience depending on the context within which the drug is taken.]
The general consensus in the scientific and medical literature is that MDMA impairs the body's ability to thermoregulate. In the rat, the ambient temperature set-point for whether a hyperthermic reaction to MDMA is observed or not seems to be 20-22C, and small incremental increases in environmental temperature above this point result in matched increases in the hyperthermic response, and corresponding reductions in brain serotonin levels. It is also interesting that MDMA must be administered peripherally and subsequently metabolized in order for any long-term alterations to the serotonergic system to occur: direct injection of the drug into the brain does not have any neurotoxic-like effects. It is now thought that metabolism of MDMA results in the formation of unstable free radicals that can target serotonergic neurons and that increased body temperature facilitates this process. But how does MDMA affect body temperature?
(1) Central effects of serotonin and dopamine on specific regions of the brain have both been implicated in the thermoregulatory effects of MDMA, as have peripheral effectors. One of these is (2) skeletal muscle thermogenesis, whereby muscle cells in our arms or legs generate huge amounts of heat via shivering and other mechanisms. [One of these is similar to brown fat thermogenesis, which I love! It's a little bit complicated but worth the diversion...so, brown fat is a certain kind of fat that can produce vast quantities of heat. It is especially prevalent in newborn babies and hibernating mammals, but adult humans retain relatively little brown fat tissue. Normally within cells, energy is produced via a specific process that involves formation of an electrochemical gradient (similar to that seen across cell membranes to produce the resting membrane potential; see here). However, in brown fat tissue, this gradient is disengaged from energy production to yield heat. Skeletal muscle cells also demonstrate this process, which is believed to be triggered by specific hormones and neurotransmitters that can be released by MDMA.] The drug dantrolene, which is the primary pharmacological line of defence in hospitalizations for MDMA-induced hyperthermia, targets one of these mechanisms, but is not always effective. The (3) endocrine system has also been implicated, in particular the thyroid hormones and some released by the pituitary and adrenal glands, as they are important in the regulation of metabolism and thermoregulation. (4) Vasoconstriction, or the narrowing of blood vessels, is another important factor. Widening of blood vessels, which allows dissipation of heat from the surface of the skin due to the increased amount of blood being transported towards the surface (the reason why we flush bright red when we are hot), is one of the ways that our body cools us down. MDMA interferes with this mechanism, an effect that has also been observed in rats and rabbits - in rats, the tail is one of the primary heat dissipation effectors, and has a rich blood supply. However, the expected increase in tail temperature is not observed following MDMA administration, despite a raised core body temperature.
The general consensus in the scientific and medical literature is that MDMA impairs the body's ability to thermoregulate. In the rat, the ambient temperature set-point for whether a hyperthermic reaction to MDMA is observed or not seems to be 20-22C, and small incremental increases in environmental temperature above this point result in matched increases in the hyperthermic response, and corresponding reductions in brain serotonin levels. It is also interesting that MDMA must be administered peripherally and subsequently metabolized in order for any long-term alterations to the serotonergic system to occur: direct injection of the drug into the brain does not have any neurotoxic-like effects. It is now thought that metabolism of MDMA results in the formation of unstable free radicals that can target serotonergic neurons and that increased body temperature facilitates this process. But how does MDMA affect body temperature?
(1) Central effects of serotonin and dopamine on specific regions of the brain have both been implicated in the thermoregulatory effects of MDMA, as have peripheral effectors. One of these is (2) skeletal muscle thermogenesis, whereby muscle cells in our arms or legs generate huge amounts of heat via shivering and other mechanisms. [One of these is similar to brown fat thermogenesis, which I love! It's a little bit complicated but worth the diversion...so, brown fat is a certain kind of fat that can produce vast quantities of heat. It is especially prevalent in newborn babies and hibernating mammals, but adult humans retain relatively little brown fat tissue. Normally within cells, energy is produced via a specific process that involves formation of an electrochemical gradient (similar to that seen across cell membranes to produce the resting membrane potential; see here). However, in brown fat tissue, this gradient is disengaged from energy production to yield heat. Skeletal muscle cells also demonstrate this process, which is believed to be triggered by specific hormones and neurotransmitters that can be released by MDMA.] The drug dantrolene, which is the primary pharmacological line of defence in hospitalizations for MDMA-induced hyperthermia, targets one of these mechanisms, but is not always effective. The (3) endocrine system has also been implicated, in particular the thyroid hormones and some released by the pituitary and adrenal glands, as they are important in the regulation of metabolism and thermoregulation. (4) Vasoconstriction, or the narrowing of blood vessels, is another important factor. Widening of blood vessels, which allows dissipation of heat from the surface of the skin due to the increased amount of blood being transported towards the surface (the reason why we flush bright red when we are hot), is one of the ways that our body cools us down. MDMA interferes with this mechanism, an effect that has also been observed in rats and rabbits - in rats, the tail is one of the primary heat dissipation effectors, and has a rich blood supply. However, the expected increase in tail temperature is not observed following MDMA administration, despite a raised core body temperature.
So, how dangerous is ecstasy?
Well, it's impossible to say for certain. It's been estimated that 12-15 people die each year from the drug in the UK, but as well over 500,000 individuals consume the drug every week, it is difficult to argue that MDMA is highly toxic, at least in the short-term. As I mentioned earlier, however, its long-term effects are very much a cause for concern.
The problem with ecstasy, and indeed, all drugs of abuse, is the idiosyncratic nature of drug-associated adverse effects. It is impossible to predict how an individual will react to a drug, and previously unsuspected underlying pathologies (affecting the cardiovascular system, in particular) could trigger a serious adverse reaction. In addition, as illegal drugs are unregulated and are cut with any number of agents, consumption is extremely risky. I hate to preach, and that's not what these essays are for really, but I would advise caution - our bodies and minds are precious and we should be wary of what we expose them to. It is difficult to think about the negative consequences when plenty of people around us seem to be taking drugs, without any apparent ill-effects, but your brain and serotonergic system will no doubt thank you in years to come if you steer clear of unregulated pharmaceuticals...
The problem with ecstasy, and indeed, all drugs of abuse, is the idiosyncratic nature of drug-associated adverse effects. It is impossible to predict how an individual will react to a drug, and previously unsuspected underlying pathologies (affecting the cardiovascular system, in particular) could trigger a serious adverse reaction. In addition, as illegal drugs are unregulated and are cut with any number of agents, consumption is extremely risky. I hate to preach, and that's not what these essays are for really, but I would advise caution - our bodies and minds are precious and we should be wary of what we expose them to. It is difficult to think about the negative consequences when plenty of people around us seem to be taking drugs, without any apparent ill-effects, but your brain and serotonergic system will no doubt thank you in years to come if you steer clear of unregulated pharmaceuticals...
