Theories of Drug Addiction
Introduction
Here, I am going to discuss several biological and psychological drug addiction theories that have been proposed by various preclinical research groups around the world. There is some overlap between them, and it is more than likely the case that it is the specific combination of some of their individual features that comes closest to most accurately representing the reality of addiction, despite their apparently dissimilar approaches. Before you begin, I have to warn you that this is a long one...I love it all so very much, and I want to make it as accessible as possible, so there's a LOT of text (obviously, it's all fabulous!). Saying that, however, it is by no means an exhaustive account, and I have just focused on the theories that I am most familiar with from my research work. Enjoy!
Some perspective...
It has become increasingly popular to attempt to use neuroscience research and our knowledge of the brain to explain all manner of ailments. Neuroscience aficionados believe that all of our thoughts, feelings, memories, and behaviours can be explained by neurochemical signalling, and that all human characteristics and emotions have a quantifiable biological basis. This movement has gained tremendous momentum in the last 15 years or so, with an explosion in the number of neuroimaging and other techniques employed, and growing technological resources. However, I sense that a backlash is imminent, as human beings are not preprogrammed robots (!), and (in my personal opinion) a lot of biological research can be somewhat ambiguous, and open to subjective interpretation.
I have been reflecting on this a lot lately, as I have left my science research days behind me and am no longer immersed in that environment. I worked in the area of drug addiction, and specifically, in the investigation of its underlying biological basis. Neuroscience has become an increasingly important research focus in this area, and addiction is now defined by many as a 'brain disorder' (despite the inverted commas, I don't think this is a bad thing at all). It is even included in the DSM-IV (soon to be V), the handbook used by medical professionals to diagnose and treat psychiatric and affective disorders. While, on the one hand, it is wonderful to see addiction being accepted as a bona-fide illness with biological features, we must also be careful not to promote a 'victim' mentality, whereby an individual thinks that he/she has no control over the addiction process, and that biological determinants are insurmountable. I probably sound like a broken record at this stage, but addiction is far more complex than this, and is a product of more than just 'bad genes' or a malfunctioning brain (and anyway, who decides what is 'bad' or 'malfunctioning'?).
Saying this, I do applaud the amazing neuroscience research that has been undertaken in this area, and I particularly admire the preclinical data showing that only a subset of animals become truly addicted to drugs. This closely resembles what we see in humans, whereby only a minority of drug-taking individuals will eventually become addicted, and therefore validates the animal models used in research. In addition, the fact that this phenomenon also occurs in animals demonstrates that addiction is not just a human construct, and for sure, a very strong biological predisposition can exist that is independent of other factors. At some point, drug-taking passes from being a voluntary, enjoyable, controlled experience to an obsession that cannot be sated, and this is very probably mediated by changes in the brain. But! Unlike rat experiments where the animal is allowed to freely self-administer the drug [note: in addiction models, self-administration techniques are generally used, whereby the animal consumes the drug as desired. For drugs such as cocaine or heroin, animals can be fitted with intravenous catheters that are attached to drug-filled syringes. These are controlled by a pump that administers a fixed amount of the drug when the animal produces the required response within a specialized experimental set-up called an operant chamber. These responses are usually lever-presses or nose-pokes], human beings experience all kinds of obstacles that prevent this, and are generally aware of the consequences of taking drugs before they try them. Therefore, humans make a CHOICE as to whether or not to try drugs or continue using them, which is determined by a number of factors, including how they feel about drugs, how educated they are about their adverse effects, and what the individual's place in society is (of course, the neuroscientists would say that all of this has already been pre-ordained by individual biological variations. You can't win!). In essence, I think animal models are fantastic for de-stigmatizing addiction, and allowing academic exploration of the underlying mechanisms, but they are inherently flawed – despite their cleverness – because humans have prior knowledge of the effects of drugs and their living environment is exponentially more complicated than animal subjects'. So what about clinical studies, using real-life human beings? Well, human studies can be difficult to interpret, cannot be fully controlled, and are usually retrospective. Again, though, they have proved incredibly useful in removing the stigma of addiction, and have led to all kinds of treatments and therapies (some more useful than others, but still).
So, with this (not so brief) disclaimer behind me, I will now give an overview of the main preclinical theories out there, and you can make up your own mind! First of all, however, I'll write a little about the reward pathway in the brain and how it relates to addiction, as this will give you a better appreciation of the different theories.
I have been reflecting on this a lot lately, as I have left my science research days behind me and am no longer immersed in that environment. I worked in the area of drug addiction, and specifically, in the investigation of its underlying biological basis. Neuroscience has become an increasingly important research focus in this area, and addiction is now defined by many as a 'brain disorder' (despite the inverted commas, I don't think this is a bad thing at all). It is even included in the DSM-IV (soon to be V), the handbook used by medical professionals to diagnose and treat psychiatric and affective disorders. While, on the one hand, it is wonderful to see addiction being accepted as a bona-fide illness with biological features, we must also be careful not to promote a 'victim' mentality, whereby an individual thinks that he/she has no control over the addiction process, and that biological determinants are insurmountable. I probably sound like a broken record at this stage, but addiction is far more complex than this, and is a product of more than just 'bad genes' or a malfunctioning brain (and anyway, who decides what is 'bad' or 'malfunctioning'?).
Saying this, I do applaud the amazing neuroscience research that has been undertaken in this area, and I particularly admire the preclinical data showing that only a subset of animals become truly addicted to drugs. This closely resembles what we see in humans, whereby only a minority of drug-taking individuals will eventually become addicted, and therefore validates the animal models used in research. In addition, the fact that this phenomenon also occurs in animals demonstrates that addiction is not just a human construct, and for sure, a very strong biological predisposition can exist that is independent of other factors. At some point, drug-taking passes from being a voluntary, enjoyable, controlled experience to an obsession that cannot be sated, and this is very probably mediated by changes in the brain. But! Unlike rat experiments where the animal is allowed to freely self-administer the drug [note: in addiction models, self-administration techniques are generally used, whereby the animal consumes the drug as desired. For drugs such as cocaine or heroin, animals can be fitted with intravenous catheters that are attached to drug-filled syringes. These are controlled by a pump that administers a fixed amount of the drug when the animal produces the required response within a specialized experimental set-up called an operant chamber. These responses are usually lever-presses or nose-pokes], human beings experience all kinds of obstacles that prevent this, and are generally aware of the consequences of taking drugs before they try them. Therefore, humans make a CHOICE as to whether or not to try drugs or continue using them, which is determined by a number of factors, including how they feel about drugs, how educated they are about their adverse effects, and what the individual's place in society is (of course, the neuroscientists would say that all of this has already been pre-ordained by individual biological variations. You can't win!). In essence, I think animal models are fantastic for de-stigmatizing addiction, and allowing academic exploration of the underlying mechanisms, but they are inherently flawed – despite their cleverness – because humans have prior knowledge of the effects of drugs and their living environment is exponentially more complicated than animal subjects'. So what about clinical studies, using real-life human beings? Well, human studies can be difficult to interpret, cannot be fully controlled, and are usually retrospective. Again, though, they have proved incredibly useful in removing the stigma of addiction, and have led to all kinds of treatments and therapies (some more useful than others, but still).
So, with this (not so brief) disclaimer behind me, I will now give an overview of the main preclinical theories out there, and you can make up your own mind! First of all, however, I'll write a little about the reward pathway in the brain and how it relates to addiction, as this will give you a better appreciation of the different theories.
The reward pathway
A specific pathway in the brain has been identified as being one of the main targets for drugs of abuse, and is responsible for the pleasurable or 'reinforcing' effects of such drugs. This is known as the reward pathway, and consists of a number of discrete brain regions that are anatomically connected, and various neurotransmitters (these are chemical messengers within the nervous system that act to relay signals between neurons, the building blocks of nervous tissue. See my earlier essay for more detail on the nervous system). What is interesting is that this pathway also mediates the pleasurable effects of activities that are within the normal behavioural repertoire of humans, such as feeding or sex, and which are essential for survival of the individual or the species. Therefore, drugs of abuse interact with an immensely powerful biological system, and consequently, their effects can be incredibly difficult to negate. The most important of these brain regions is the nucleus accumbens, located in the striatum, and dopamine is the neurotransmitter responsible for mediating 'pleasure' (it is also known as the 'hedonistic neurotransmitter'). All drugs of abuse, no matter how disparate, increase the levels of dopamine in the nucleus accumbens – without this effect it is fairly safe to say that a drug will not be abused. A second important brain region is the ventral tegmental area, and the connection between this region and the nucleus accumbens (among other areas) is known as the mesolimbic pathway. This is the crux of the reward mechanism within the brain, and therefore, a major focus for addiction research groups [if you REALLY like the sound of all of this, check out the Wikipedia entry on the mesolimbic pathway – it's very good!].
Note: In the interests of brevity, I have only superficially touched on dopamine and its role in pleasure and reward. The exact nature of this relationship is a massive research area in its own right, and I have written more about it in my blog post here, which is in essence an elaboration of Theory Number 2 below.
Note: In the interests of brevity, I have only superficially touched on dopamine and its role in pleasure and reward. The exact nature of this relationship is a massive research area in its own right, and I have written more about it in my blog post here, which is in essence an elaboration of Theory Number 2 below.
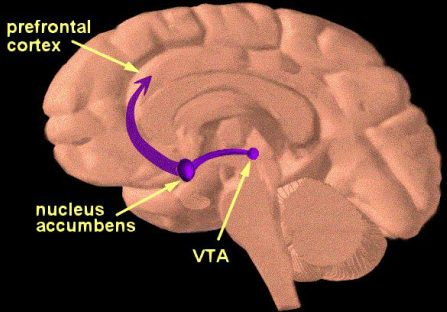
This section through the brain (the front is to the left, the back is to the right) shows the ventral tegmental area (VTA) and the nucleus accumbens, both of which are hugely important brain regions in addiction research (picture taken from the NIDA website, www.drugabuse.gov)
The theories...
1. Self-Medication Hypothesis
I've already referred to the Self-Medication Hypothesis, developed by Edward Khantzian and David Duncan in the 1970s, so I won't dwell on it for too long. Basically, it maintains that drug-abusing individuals are self-medicating specific problems or defects, and that the pharmacological effects of drugs are used to treat underlying biological deficits or abnormalities (for example, an individual could have innate alterations in a certain neurotransmitter system that results in feelings of anxiety. Alcohol, which targets the same system, 'normalizes' this biological impairment, and makes the individual feel better). I like this very much, and think it is an excellent starting-point, but I also have various issues with it, and I don't believe it adequately explains addiction as such. However, it was the first attempt to develop a holistic and scientific viewpoint of addiction, and is remarkable for that alone.
2. Incentive Salience
The Incentive-Sensitization Theory, developed by the researchers Terry Robinson and Ken Berridge in 1993, holds that repeated exposure to addictive drugs results in sensitization of the dopaminergic mesolimbic reward pathways in the brain (which we looked at earlier), leading to an increased desire or craving for the drug - that is, there is a perceived increase in the value of the drug or an enhancement of its 'incentive value'. This theory proposes that otherwise neutral environmental stimuli come to acquire ‘incentive salience’ when repeatedly paired with drug administration, through the process of classical or Pavlovian conditioning (where repeated association of a cue with a reward will make the cue desirable in its own right, even in the absence of the reward). In addition, Robinson and Berridge make a further distinction between ‘liking’ the drug and ‘wanting’ the drug. They propose that changes in the neural systems underlying incentive salience (that is, ‘wanting’) can occur independently of changes in neural systems responsible for both mediating the pleasurable subjective effects of the drug (‘liking’) and the aversive effects of drug withdrawal. Consequently, drug-associated stimuli can be sufficient to produce compulsive addictive behaviour despite diminished expectation of the pleasurable effects of the drug, and regardless of the negative consequences of such behaviour, including relationship breakdown or job loss. Drug-related cues can also precipitate 'craving' and relapse to drug abuse, long after the discontinuation of drug use.
3. The 'Dark Side' of Addiction: Antireward
Developed by Michel Le Moal, Serge Ahmed, and George Koob, this focuses on the negative reinforcing effects of drugs, or how they are used to relieve physical and psychological withdrawal symptoms. A key element of the addiction process is the development of a negative emotional state during drug withdrawal or abstinence. It is believed by proponents of the Antireward Theory that excessive activation of the reward pathway results in the recruitment of brain stress and emotional systems, which is the body's attempt to ensure stability. In this regard, homeostasis is a self-regulating process that acts to maintain body parameters around a set-point critical for survival (in response to an acute challenge) while allostasis maintains stability outside the normal homeostatic range, where an organism must vary all the parameters of its physiological systems to match them appropriately to chronic demands. In other words, allostasis is a process of maintaining stability or ‘apparent stability’ through change, but this occurs at a price. In this model, therefore, drug addiction represents an allostatic adaptation. Specifically, chronic dysregulation of reward neurotransmitters, and the subsequent chronic recruitment of antireward neurotransmitters in order to balance this, leads to a change in what is called the hedonic set-point. The hedonic set-point is unique for every individual and refers to our threshold for experiencing the pleasurable effects of rewards: a low hedonic set-point effectively means that small rewards make an individual quite happy, while those with a higher set-point require much greater rewards to feel the same effect. This theory has been used to explain why addicts need increased amounts of a drug in order to feel the same 'high'.
4. Habit Formation
The 'Habit Formation' or Compulsive Theory is based on pioneering work carried out by Bernard Balleine and Anthony Dickinson in 1998, who first characterised instrumental learning [instrumental learning in animals refers to learning to lever-press or nose-poke for drug or food rewards – a behaviour that is not 'normal' for the animal to undertake – and is distinct from innate or Pavlovian instinctual behaviour, where the individual simply responds to the environment. Drug-taking in humans is a form of instrumental learning] as comprising two separate components. These are a goal-directed process, whereby the individual is consciously aware of what he/she is doing and will only carry out the desired action if the reward is of considerable value (for example, the reinforcing 'high' resulting from drug use), and what they called a stimulus-response or habit mechanism, whereby the objective value of the reward is irrelevant – the individual is carrying out the action without thinking of the real consequences of this action, or if the reward is even worth it any more; that is, it has become COMPULSIVE and is not amenable to any kind of subjective assessment. Stimulus-response refers to cues (these are the stimuli) that trigger an automatic response, which the individual cannot control. The addiction theory of Trevor Robbins and Barry Everitt from the University of Cambridge (this was my lab!) holds that drug addiction represents a transition from goal-directed behaviour to stimulus-response behaviour, reflecting a shift in brain regional control over drug-seeking (different parts of the brain mediate these two types of behaviour). This is pretty profound stuff and I hope I've managed to explain it properly. It is super-cool, though!
I've already referred to the Self-Medication Hypothesis, developed by Edward Khantzian and David Duncan in the 1970s, so I won't dwell on it for too long. Basically, it maintains that drug-abusing individuals are self-medicating specific problems or defects, and that the pharmacological effects of drugs are used to treat underlying biological deficits or abnormalities (for example, an individual could have innate alterations in a certain neurotransmitter system that results in feelings of anxiety. Alcohol, which targets the same system, 'normalizes' this biological impairment, and makes the individual feel better). I like this very much, and think it is an excellent starting-point, but I also have various issues with it, and I don't believe it adequately explains addiction as such. However, it was the first attempt to develop a holistic and scientific viewpoint of addiction, and is remarkable for that alone.
2. Incentive Salience
The Incentive-Sensitization Theory, developed by the researchers Terry Robinson and Ken Berridge in 1993, holds that repeated exposure to addictive drugs results in sensitization of the dopaminergic mesolimbic reward pathways in the brain (which we looked at earlier), leading to an increased desire or craving for the drug - that is, there is a perceived increase in the value of the drug or an enhancement of its 'incentive value'. This theory proposes that otherwise neutral environmental stimuli come to acquire ‘incentive salience’ when repeatedly paired with drug administration, through the process of classical or Pavlovian conditioning (where repeated association of a cue with a reward will make the cue desirable in its own right, even in the absence of the reward). In addition, Robinson and Berridge make a further distinction between ‘liking’ the drug and ‘wanting’ the drug. They propose that changes in the neural systems underlying incentive salience (that is, ‘wanting’) can occur independently of changes in neural systems responsible for both mediating the pleasurable subjective effects of the drug (‘liking’) and the aversive effects of drug withdrawal. Consequently, drug-associated stimuli can be sufficient to produce compulsive addictive behaviour despite diminished expectation of the pleasurable effects of the drug, and regardless of the negative consequences of such behaviour, including relationship breakdown or job loss. Drug-related cues can also precipitate 'craving' and relapse to drug abuse, long after the discontinuation of drug use.
3. The 'Dark Side' of Addiction: Antireward
Developed by Michel Le Moal, Serge Ahmed, and George Koob, this focuses on the negative reinforcing effects of drugs, or how they are used to relieve physical and psychological withdrawal symptoms. A key element of the addiction process is the development of a negative emotional state during drug withdrawal or abstinence. It is believed by proponents of the Antireward Theory that excessive activation of the reward pathway results in the recruitment of brain stress and emotional systems, which is the body's attempt to ensure stability. In this regard, homeostasis is a self-regulating process that acts to maintain body parameters around a set-point critical for survival (in response to an acute challenge) while allostasis maintains stability outside the normal homeostatic range, where an organism must vary all the parameters of its physiological systems to match them appropriately to chronic demands. In other words, allostasis is a process of maintaining stability or ‘apparent stability’ through change, but this occurs at a price. In this model, therefore, drug addiction represents an allostatic adaptation. Specifically, chronic dysregulation of reward neurotransmitters, and the subsequent chronic recruitment of antireward neurotransmitters in order to balance this, leads to a change in what is called the hedonic set-point. The hedonic set-point is unique for every individual and refers to our threshold for experiencing the pleasurable effects of rewards: a low hedonic set-point effectively means that small rewards make an individual quite happy, while those with a higher set-point require much greater rewards to feel the same effect. This theory has been used to explain why addicts need increased amounts of a drug in order to feel the same 'high'.
4. Habit Formation
The 'Habit Formation' or Compulsive Theory is based on pioneering work carried out by Bernard Balleine and Anthony Dickinson in 1998, who first characterised instrumental learning [instrumental learning in animals refers to learning to lever-press or nose-poke for drug or food rewards – a behaviour that is not 'normal' for the animal to undertake – and is distinct from innate or Pavlovian instinctual behaviour, where the individual simply responds to the environment. Drug-taking in humans is a form of instrumental learning] as comprising two separate components. These are a goal-directed process, whereby the individual is consciously aware of what he/she is doing and will only carry out the desired action if the reward is of considerable value (for example, the reinforcing 'high' resulting from drug use), and what they called a stimulus-response or habit mechanism, whereby the objective value of the reward is irrelevant – the individual is carrying out the action without thinking of the real consequences of this action, or if the reward is even worth it any more; that is, it has become COMPULSIVE and is not amenable to any kind of subjective assessment. Stimulus-response refers to cues (these are the stimuli) that trigger an automatic response, which the individual cannot control. The addiction theory of Trevor Robbins and Barry Everitt from the University of Cambridge (this was my lab!) holds that drug addiction represents a transition from goal-directed behaviour to stimulus-response behaviour, reflecting a shift in brain regional control over drug-seeking (different parts of the brain mediate these two types of behaviour). This is pretty profound stuff and I hope I've managed to explain it properly. It is super-cool, though!
Conclusions
So, there you have it! Drug addiction is not easy to understand, but preclinical research has shed some light on this complex disorder, even if the theories are still evolving. As I mentioned previously, it is unlikely that one of these provides the Ultimate Answer, and instead, it is probably an amalgamation of all these theories that most closely resembles human drug addiction. Consequently, an integrated model will hopefully give us an even greater insight into this disorder.
For me, the most fascinating aspect of the process is how individuals CAN stop taking drugs and reclaim their lives: this cannot be modelled in the laboratory and is inadequately addressed by the biological theories of addiction. Instead, it speaks volumes for the enduring nature and sheer force of the human spirit, and emphasizes that we are far more than the sum of our biological parts. Nobody is beyond redemption and addiction is entirely treatable, with the correct support and motivation to do so. Neuroscience and biology are not the be all and end all; science provides a mechanism whereby we can attempt to understand a problem, but it is just one piece of the jigsaw puzzle, and its reach should not be overestimated: not everything can be measured in a laboratory!
For me, the most fascinating aspect of the process is how individuals CAN stop taking drugs and reclaim their lives: this cannot be modelled in the laboratory and is inadequately addressed by the biological theories of addiction. Instead, it speaks volumes for the enduring nature and sheer force of the human spirit, and emphasizes that we are far more than the sum of our biological parts. Nobody is beyond redemption and addiction is entirely treatable, with the correct support and motivation to do so. Neuroscience and biology are not the be all and end all; science provides a mechanism whereby we can attempt to understand a problem, but it is just one piece of the jigsaw puzzle, and its reach should not be overestimated: not everything can be measured in a laboratory!
